
|
|
|
« Back to Action Center
How is the Series Being Used with External Groups? 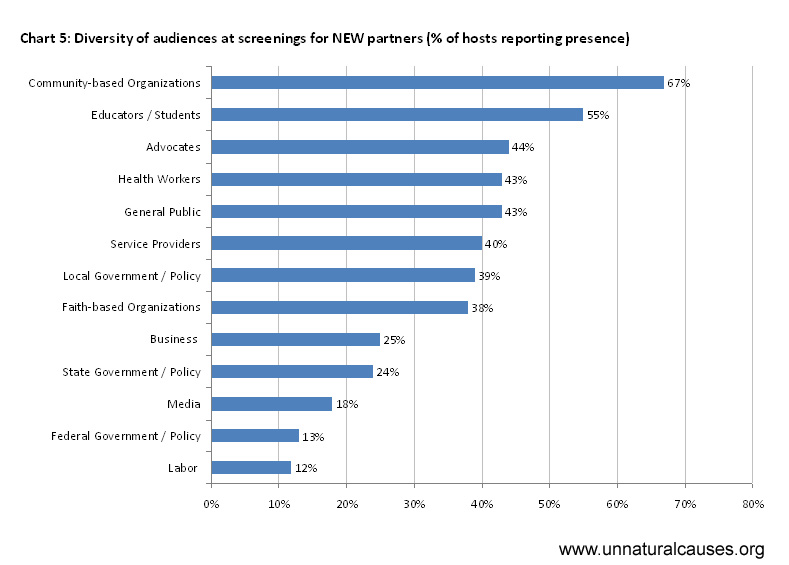 Chart 5: Diversity of audiences at screenings for new partners Chart 5: Diversity of audiences at screenings for new partners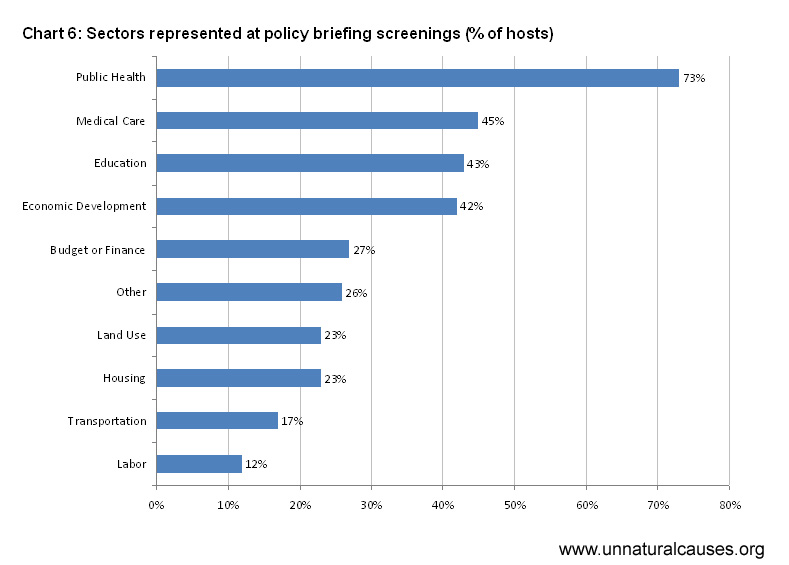 Chart 6: Sectors represented at policy briefing screenings Chart 6: Sectors represented at policy briefing screenings Chart 7: External screenings helped audiences understand that... Chart 7: External screenings helped audiences understand that... 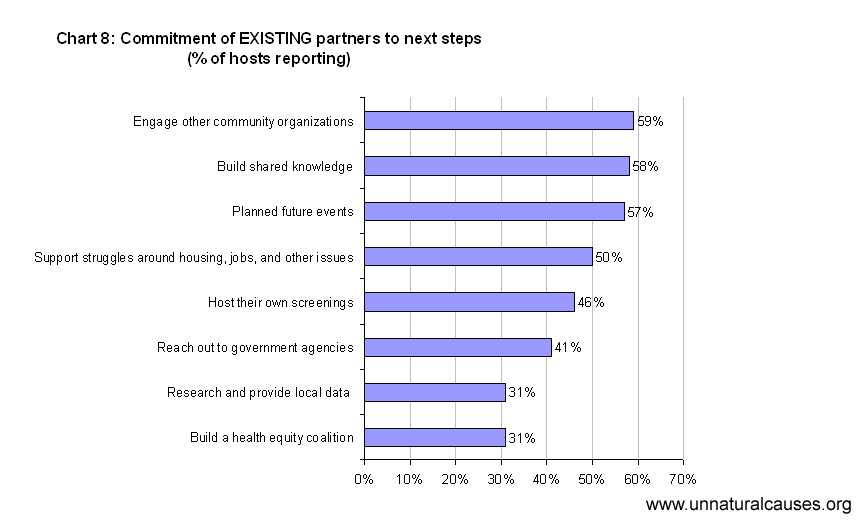 Chart 8: Commitment of existing partners to next steps Chart 8: Commitment of existing partners to next steps
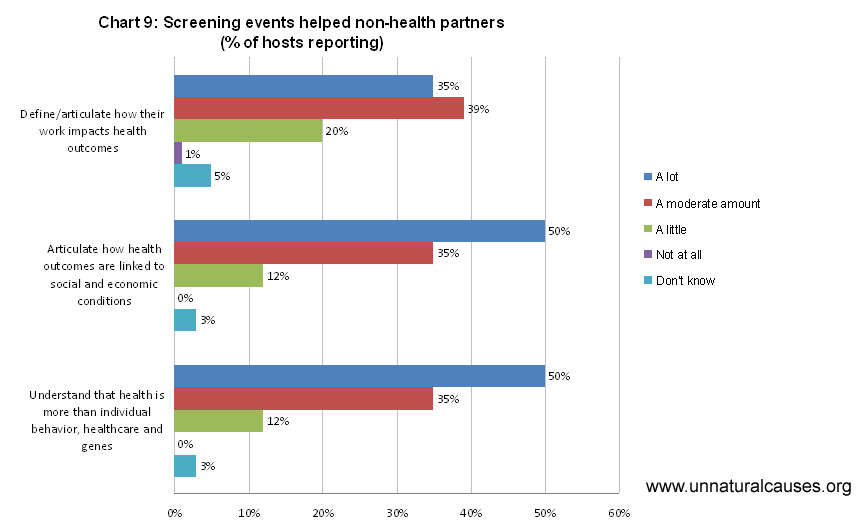 Chart 9: Screening events helped "non-health" partners... Chart 9: Screening events helped "non-health" partners...
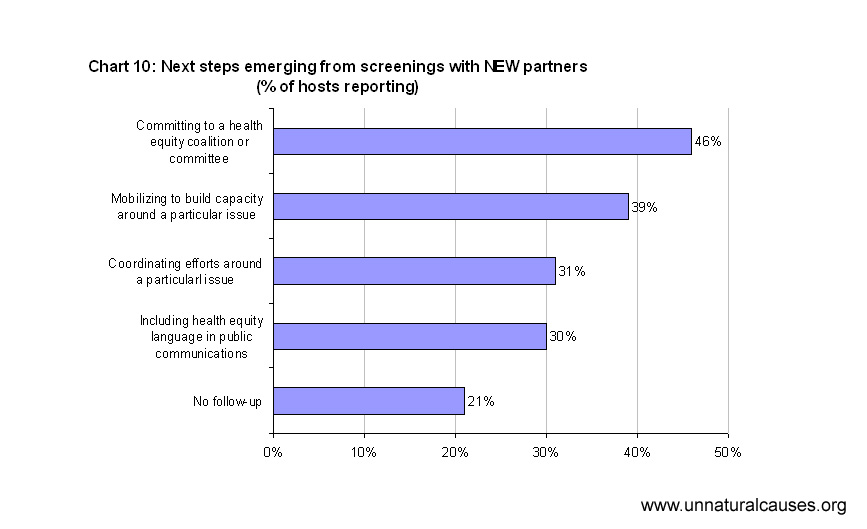 Chart 10: Next steps
emerging with new partners Chart 10: Next steps
emerging with new partners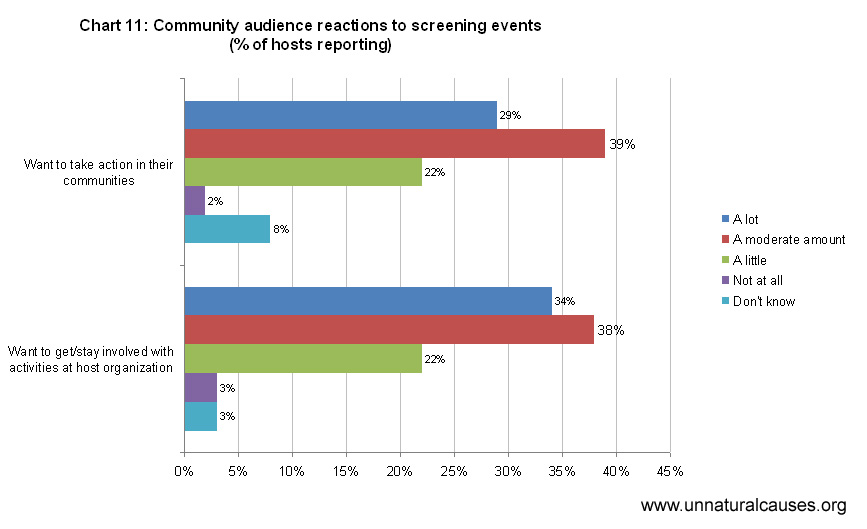 Chart 11: Audience reactions at community screenings Chart 11: Audience reactions at community screenings Screenings With New or Existing Partners: A little over half the respondents (55%) had used the series with their existing allies. Of those, 35% engaged one to three existing partners, while 27% engaged ten or more partners in their screenings, potentially setting the groundwork for a broader coalition or alliance. Regarding their partners’ areas of interest, 38% of hosts reported that “most” of their partners worked in health care while 30% said “most” worked to address the social determinants of health. More than a third (37%) of respondents used the series to create new alliances with organizations. Of those, three fourths (74%) reported that it had been “very easy” or “moderately easy” to engage members from other sectors on the planning team. Audiences attending alliance-building external screenings most frequently included representatives of community-based organizations, educators and students, and advocacy organizations (Chart 5). Representatives from labor, federal government, and media were least often represented. With Community Members Half of the organizations surveyed (50%) screened the series for community members. Most (76%) planned their events in partnership with other organizations and 73% invited other community agencies to table and share resources at the event. With Policymakers and Elected OfficialsThe majority of respondents indicated that they believed public policy change was important, but by the time of the survey only a fifth had already used the series as part of briefings with policymakers and governments officials such as city council members, legislators, department directors, and agency or legislative staff. Most of the groups who had successfully engaged policymakers and elected official did so at the municipal level (80%), although many also worked at the state level (42%) and some reached policymakers at the federal level (10%). Groups most often targeted policymakers and elected officials in public health, medical care, education, and economic development (See Chart 6). Groups least often reached out to representatives of transportation and labor.
Attitude Changes from External Screenings: Perhaps unsurprisingly, external audiences had more trouble that internal audiences in breaking through the prevailing individual bio-medical paradigm and making the connection between social and economic policies as health policies.Revealingly, community groups seemed most open to these messages, while policymakers were most resistant.
Actions and Next Steps With New or Current Partners Most organizations believed that their screening event helped new allies working in non-health sectors “a lot” or “a moderate amount” to articulate how health outcomes are linked to social and economic conditions and to define/articulate how their work impacts health (Chart 9). Commitments from new partners were similar to those from existing partners, though one fifth of respondents indicated that no follow-ups steps emerged from their screenings (Chart 10). Screenings with the Community The majority of hosts reported that they provided community members with
Of respondents who reported that actions steps emerged from their community screenings, only half provided specific information on the action steps. These steps included:
The vast majority of reported action steps consisted of encouraging audiences to educate others about the social determinants of health, and examples reported for potential actions tended to be very general, such as:
When asked about follow up activities, 48% of those organizing community screenings reported that they had not planned any, possibly indicating that their screenings were organized as one-time educational events rather than as a component of a larger health equity strategy or action plan.
Breaking free of the individual, bio-medical paradigm The survey and other research suggests that normative understandings about health (i.e., the “common sense” prism through which many people filter, interpret, and make sense of health information) are grounded in several deep-seated assumptions:
Seen through the prism of this individual, bio-medical paradigm, population health differences appear to stem from lack of access to health care or reflect the “unhealthy choices” made by “self-determining individuals,” be it from ignorance, lack of self-discipline, cultural practices, or “lifestyle” choices. Hence, health gaps are commonly seen as unfortunate but not necessarily unfair or unjust. Preconceptions are can be extremely powerful and difficult to change: It takes more than a screening to unlearn them. See our recommendations for tips on helping your audience hear and understand the evidence for the relevance of social determinants.
|
|
|||
|